Is your Behavioral Crisis Management System Really Trauma Informed?
Trauma associated with events like abuse and neglect can occur at any point in somebody’s life. Not surprisingly, these types of experiences are frequently reported by those receiving behavioral and mental health services, especially by children and adolescents in foster or residential care and individuals with developmental disabilities. Researchers and advocates frequently cite “trauma-informed care” as essentially knowing the history of past and current abuse of an individual and designing service systems that are sensitive to these traumatic experiences and directly involve the individual as a participant in the design and implementation of treatment and education.
")
Most crisis management systems focus on de-escalation, physical crisis intervention techniques, and are otherwise rooted in mainly coercive approaches.
Since the concept and term “trauma-informed care” received growing recognition, it’s not surprising there are several crisis management systems now touting trauma-informed approaches. Sure, they create amazing graphics, use warm and fuzzy words, and even develop training with titles like Trauma Informed Care approaches. But if you lift the hood and take a deeper look at the strategies used, you find these approaches are in fact, not trauma informed. Most crisis management systems focus on de-escalation, physical crisis intervention techniques, and are otherwise rooted in mainly coercive approaches. They call their de-escalation techniques ‘prevention,’ yet their 'prevention techniques’ do not start until the individual shows the first signs of escalation. If anything is linked to prevention, it might be 1 or 2 concepts, and those are glossed over.
When compared with a system that totally aligns with the Trauma Informed Care concept, such as PCM, the differences are striking. For example, prevention in the PCM system begins before the individual arrives at the facility. Detailed historical records and past evaluations are collected and used and analyzed to create a framework for real prevention through treatment and education. Nothing compares to the more than 100 prevention strategies outlined in detail in the PCM curriculum that consider both the individual’s and the practitioner’s histories.
Individuals and Families Want a Complete System that is Trauma Informed

People who struggle with behavioral and mental health issues desire approaches to crisis management grounded in positive reinforcement. So do their loved ones. They want to be treated with dignity and respect and regularly provided choices and feedback to assist in learning, even during a crisis event. And they certainly want to avoid any type of pain or distress.
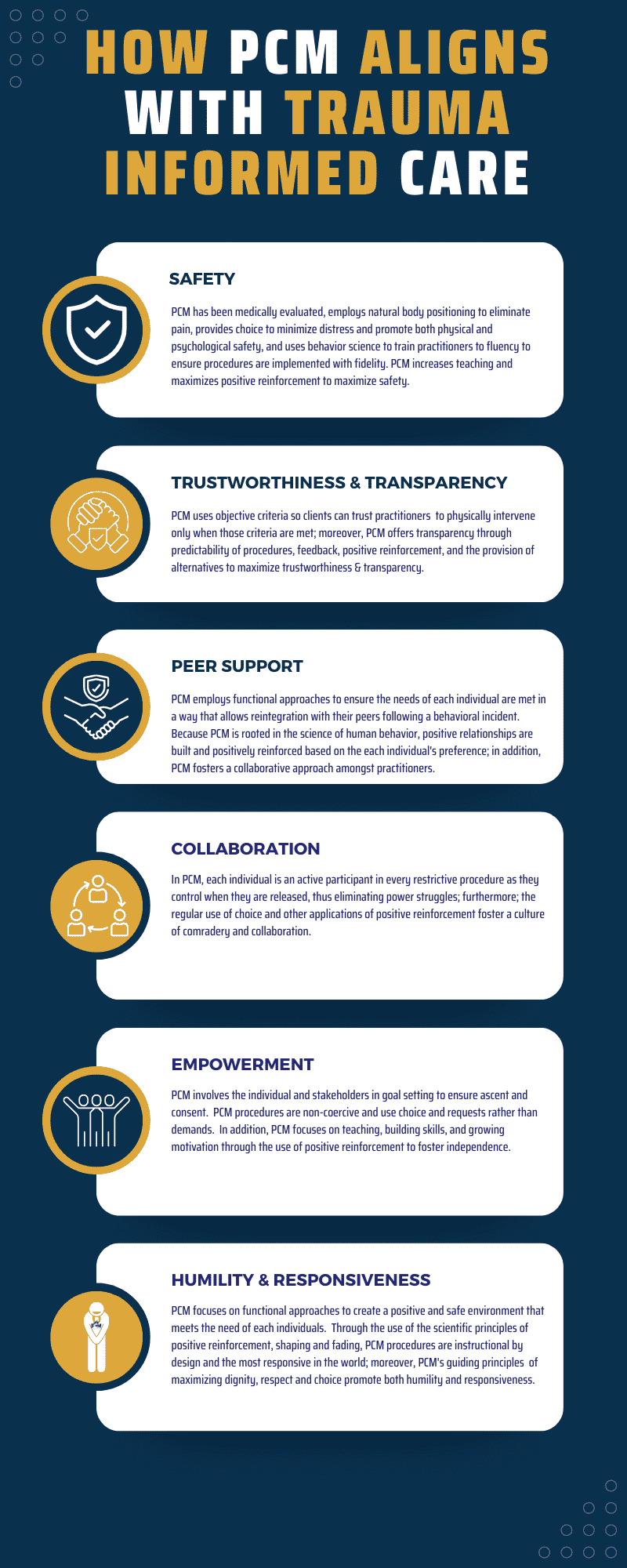
PCM offers a complete crisis management system made up of prevention, de-escalation, intervention, and reintegration that perfectly aligns with the core principles of Trauma Informed Care. This means PCM’s curriculum, instruction, guiding principles, and procedures directly aid in fostering an environment characterized by safety, trust, peer support, collaboration, empowerment, and respect.
Comparing the precise and evidenced-based PCM approach to other crisis management systems in implementing trauma-informed care is like comparing a surgeon to a paramedic. While both are well-intended professionals who examine, evaluate, and treat patients, the paramedic has general medical knowledge and limited tools aimed at getting a patient safely to the emergency room in the event of a crisis. In contrast, the surgeon, who has expertise in both averting and treating a crisis, is responsible for the preoperative diagnosis of the patient, for performing the operation, and for providing the patient with postoperative surgical care and treatment. The two just aren’t comparable. And neither are the trauma-informed approaches of PCM as compared to other crisis management systems.
Trauma Informed and Rooted in ABA Since 1981
In fact, PCM has always been trauma- informed. Traditionally, many schools and facilities take a “what’s wrong with you?” approach to addressing behavioral issues. Trauma-informed care shifts this perspective from “What’s wrong with you?” to “What happened to you?” by having a complete picture of a person’s situation and life — past and present — as means to individualize education, treatment, and support. This approach is fundamental to Applied Behavior Analysis, or ABA, as it seeks to determine the root causes of behavior based on both the current environment and the individual’s history. For example, perhaps an individual was exposed to an aversive series of events such as, as a child being regularly beaten for not completing their chores or for receiving poor grades. These past events now influence subsequent experiences with adults related to being corrected.
Technically speaking, we may be able to categorize responses to certain related environmental stimuli (e.g., an individual being reprimanded for failing to complete a task) as avoidance, response suppression, aggression, or perhaps internal responses like increased heart rate. Whatever the case, behavior analysts seek to use data from the present and the past to determine the function of the behavior and then make environmental adjustments to accommodate them. We are proud to say that, since our humble beginnings in 1981, PCM has always been rooted in ABA with emphasis on accommodating individuals with past traumas and preventing potential new traumas.

Understanding that PCM is conceptually rooted in ABA is also important because the Ethics Code for Behavior Analysts compels practitioners to not only describe the objectives of a behavior change program to clients, but to minimize potential risk in ABA practice and research and to ensure the selection of the least restrictive procedures necessary for effective treatment. All PCM’s procedures adhere closely to this code while ensuring procedures are in no way harmful, degrading, painful, or dehumanizing.
Guiding Principles of PCM and TIC

Below we will take a brief look at the 6 principles of trauma-informed care and provide some examples of PCM’s alignment with them. First, let’s review the 4 guiding principles on which all PCM procedures are built and that are closely aligned with those of trauma- informed care. These principles are:
• Maximize dignity and respect
• Eliminate pain and minimize distress
• Minimize restriction and offer choice, and
• Give feedback and provide alternatives
1.Safety
Let’s start with the first trauma informed principle, Safety. As behavior analysts, we argue safety is a prerequisite to effective treatment and education. To ensure that PCM is and remains the safest, most effective and humane crisis management solution in the world, PCM has been evaluated by a medical doctor, employs natural body positioning to eliminate pain, provides choice to minimize distress and promote both physical and psychological safety, and uses behavior science to train practitioners to fluency to ensure procedures are implemented with fidelity.
With other crisis management systems, we have seen physical procedures that can easily harm the individual when not applied exactly as prescribed, especially with individuals who are at more risk, such as those with Down Syndrome. There is no room for error. And lots of errors happen as practitioners of these systems are not trained to fluency. Not only the consumers are at risk, but the practitioners as well, especially when trying to restrain much bigger and stronger individuals. We also argue that psychological safety must be prioritized to the same degree as physical safety, and that one must not come at the expense of the other.
2. Trust and Transparency
Trust and transparency, the second principle of trauma informed care, are fundamental to psychological safety. To ensure psychological safety, PCM focuses on building trustworthiness and transparency through the regular application of positive reinforcement and using objective criteria and predictability of procedures so individuals are always aware of what is happening and what will happen next. Individuals are far more likely to “feel safe” when there is consistency and predictability that result from an accumulation of positively reinforcing interactions. In contrast, other systems that lack precision and are not primarily rooted in positive reinforcement not only fail to build trust and transparency, they have the exact opposite effect as individuals quickly begin "feeling unsafe." PCM goes further by acting as a checks and balance system for treatment systems that are ongoing for the individual.
For example, the PCM system asks each practitioner and instructor to review ongoing schedules, teaching methodologies, and curricular accommodations for each student who receives treatment and/or educational services to ensure they are practical, effective, and have integrity
3. Peer Support
The next principle of trauma informed care is peer support. PCM employs functional approaches to make certain the needs of each individual is met in a way that allows them to be reintegrated back with their peers following a behavior incident. Because PCM is rooted in the science of human behavior, positive relationships are built and reinforced based on everyone’s ability and preferences, including staff. The PCM behaviorists who built and evolved the PCM system cut their teeth transforming schools and treatment facilities throughout the ‘80s and ‘90s, resulting in a new and transformative approach to education and treatment. It wasn’t accomplished by any one behaviorist, but instead was the collaborative effort of many hundreds working together, sharing experiences, conducting cogent research, and otherwise supporting one another as peers as they steered a course to a new and better approach. The PCM system and the people involved were part of that revolution and are committed to the premise that only with peer support will we meet our goals and continue to make progress.

4. Collaboration
The fourth principle of trauma informed care is collaboration. Behavioral and educational treatments, unlike other types of interventions, may span long periods of time. For example, unlike surgery, a behavioral treatment may span weeks, months, and possibly years in more intensive situations. A behavioral treatment may involve not only professionals trained to reduce dangerous behavior and increasing academic, functional, and pro-social skills, but also caring and supporting individuals across less restrictive classrooms and living facilities. It is for this reason that PCM places such a focus on collaboration. In PCM, each individual is an active participant in every procedure, including restrictive procedures, as they are provided choices. This approach eliminates power struggles; furthermore, the regular use of choice and other applications of positive reinforcement fosters a culture of comradery and collaboration, which has positive educational and therapeutic effects. The entire PCM process is collaborative in nature. From determining a person’s needs and preferences and arranging a positively reinforcing environment to encourage success, to actively listening, making accommodations, and providing information so an individual can make the best choices for themselves, PCM engages in practices that are socially valid for both the individual and the practitioners.
In contrast, other systems that focus primarily on de-escalation and restraint, place practitioners in a position of coercion as they fail to foster a sense of well-being through the use of prevention strategies grounded in positive reinforcement. This quickly leads to individuals feeling alienated and victimized, even though this is very likely not the intent of those applying the procedures they've been taught.

5. Empowerment
The 5th principle of trauma informed care is Empowerment – Many issues associated with trauma can be linked to behavioral deficit or excess. PCM focuses on empowering individuals by first recognizing behavior deficits and behavioral excesses, and then using positive reinforcement to build skills or teach replacement behaviors as a means of helping individuals better adapt to the environment and even overcome issues associated with trauma. PCM uses continuous feedback through biofeedback to facilitate rapid learning, even during crises, and offering least restrictive alternatives to foster independence and participation in regular educational or treatment programming. In addition, PCM’s principles and procedures are built to seamlessly blend with existing treatment and educational processes as staff are empowered with the knowledge and skills to effectively teach, prevent, and safely intervene at precisely the right time, in precisely the right way.
Whether preventing a crisis or intervening in one, feedback is key to empowerment as all learning requires feedback. Other systems do not focus on building skills as a prevention strategy or do not have tight feedback loops to promote accelerated learning, even during physical interventions. As such, individuals are too frequently denied the ability to learn and grow, especially during a crisis.
6. Humility and Responsiveness
The final principal of trauma informed care is humility and responsiveness. In PCM, practitioners are not only trained to focus on building and maintaining positive relationships, but they are also trained to recognize and manage their own negative emotions; moreover, they are trained to avoid, at all costs, coercive interactions as a means of forcing compliance from individuals. Through the scientific principles of shaping and fading, combined with the most comprehensive crisis management system in existence for preventing and safely intervening during a crisis, PCM procedures are the most precise and responsive in the world.
Other systems do not train practitioners to effectively build and maximize positive relationships. Nor are practitioners provided the tools to better recognize and manage their emotions in response to behavioral issues. This can inadvertently place practitioners in a position of superiority where they become unresponsive to the needs of an individual as they perceive all behavioral issues as simply compliant or non-compliant, instead of as a form of communication to interpret and respond to.
Is your organization going to be Trauma Informed?
PCM was developed because individuals were being restrained on the hard ground within a residential facility. This resulted in injury to both the individual and those restraining them. It also increased the duration of restraints as the individual, like anybody, fought to escape due to pain. Not only did this damage therapeutic and educational relationships, but who knows what kind of impact it had on all of them psychologically? Whether they had past traumatic experiences, or these experiences were becoming traumatic, it was not good. And it wasn’t just the physical restraints that caused problems. Individuals were not involved in their own treatment and were being forced to do things they didn’t want to. They had no choice. But you do.
If you support trauma-informed care, understand this. Very difficult behavior falls into two categories: behaviors you can ignore, and behaviors that must be stopped. Even though PCM practitioners are equipped with training and procedures to stop behaviors that are dangerous to an individual or others, PCM does not advocate for the use of physical safety as a compromise to psychological safety. Just the opposite. It is why more than three quarters of our curriculum is dedicated to empowering individuals through choice, skill building, and the application of positive reinforcement as prevention strategies to avoid the use of restraint. It is also why PCM has such a wide range of physical interventions so that the least restrictive interventions, which employ natural body positioning and no pain, can be used to meet the needs of each individual across contexts.

Simplified version of a checklist used to hold a Crisis Management System against Trauma Informed Care principles.

So, as we see it, you have a simple choice to consider if you have a crisis management system, or you are thinking about one: Do you want to use imprecise and limited procedures that are considered coercive? Procedures that limit choice, feedback, and alternatives as a means of addressing crisis type behaviors? Or do you want to prevent and stop these behaviors using principles that are grounded in behavior science and directly aligned with trauma-informed care? Approaches that are physically and psychologically safe, responsive, and transparent. Approaches that otherwise empower and foster trusting and collaborative relationships. If the latter is your choice, then you need Professional Crisis Management.